AORTIC SURGERY AND STENTING
Diseases of the aorta (the largest artery in the body supplying blood from the heart to the rest of the body) are now recognised to be commoner in people of Asian descent than previously thought. They are more frequent in men and the consequences of untreated aortic disease can be catastrophic particularly when this large artery ruptures.
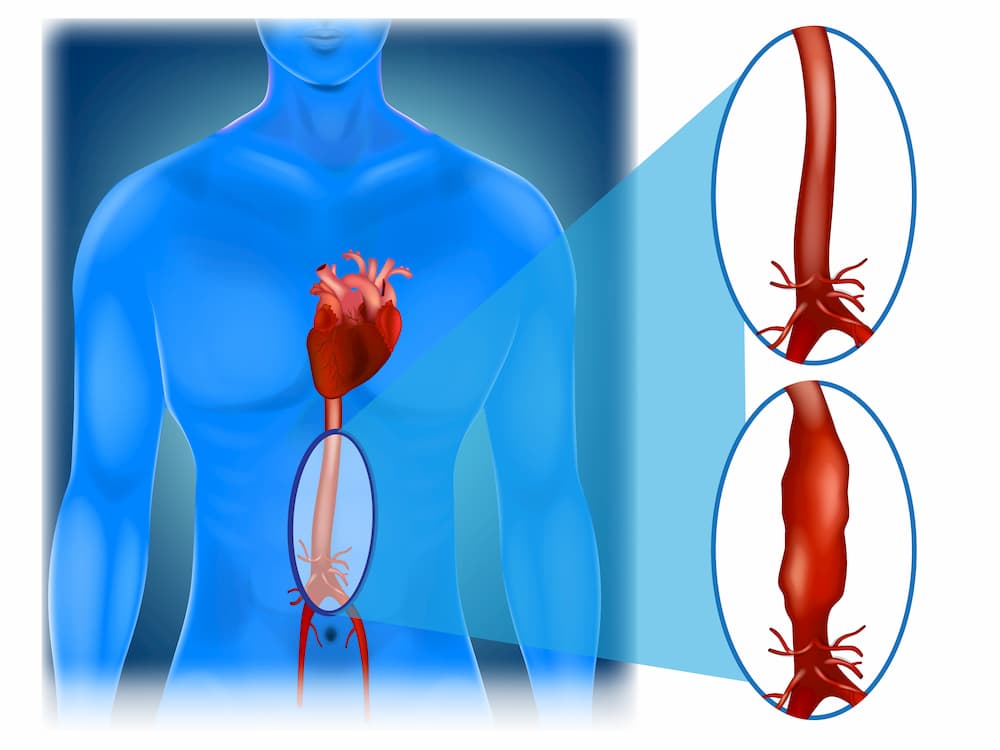
The aorta can be affected both in the chest and in the abdomen by two conditions – aortic aneurysms in which the aorta swells or balloons out due to a weakness in its wall or an aortic dissection in which the inside lining of the aorta splits leading to a rupture or a loss of blood supply to an important organ. In addition, blockages in the aorta and the arteries supplying the abdominal organs from cholesterol and calcium can also occur as in arterial disease affecting the limbs. A significant genetic link is suspected particularly in sons of fathers who may have had aneurysms. Our aortic aneurysm screening programme allows these conditions to be detected early.
Our vascular surgery service offers both endovascular (keyhole) repair with stents as well as traditional open surgical repair (for patients unsuitable for endovascular surgery) for all types of aortic disease. In addition, the support of our specialist cardiologists to optimise the co-existing problems of heart disease and blood pressure is crucial to ensuring the best outcomes for patients undergoing such major surgery.
If you or a member of your family have had an aortic aneurysm, or if you suffer from hypertension, are a smoker or you would like a vascular health or aortic aneurysm screen, contact us or visit the relevant pages of this website for more information.
- Abdominal Endovascular aneurysm repair (EVAR) An EVAR is an endovascular (keyhole) procedure carried out to repair a diseased aorta that lies within the abdomen. It is performed under general anaesthesia via a small 1-2 cm cut in each groin. Stents are then carefully placed via the leg (femoral) artery to re-line the inside of the diseased segment of the aorta with a stent covered with fabric (a tube within a tube). This takes the pressure off the diseased aortic wall and prevents a rupture from occurring.
Sometimes additional stents to protect the arteries to the kidneys (renal arteries) or the gut (mesenteric artery) are required and these are called chimney stents. Custom made stents may also be needed in some cases, called fenestrated stents. These more complex procedure may especially be needed in Asian patients when more standard stents cannot be used. - Thoracic Endovascular aneurysm repair (TEVAR) This is similar to an EVAR procedure except that the diseased aorta is within the chest cavity. Stents are placed the diseased segment in the chest, but great care is required to protect the carotid arteries that supply blood to the brain during this procedure.
Occasionally, chimney stents or an additional surgical procedure called a carotid-carotid bypass is required to protect the carotid arteries during a TEVAR. - Open surgical repair of aortic aneurysms and aortic occlusions These major surgical procedures are fortunately not often required now if the procedure is a planned elective operation, when an endovascular repair is usually feasible. However, it may be the only option to prevent death in the event of an aortic rupture, when an emergency procedure to replace the diseased aorta with a special fabric tube called a graft is performed. These are high-risk life-saving procedures and recovery will include a short admission to an intensive care unit.
Early detection of aortic dissections and aneurysms that are at risk of rupture by screening can prevent the need for these major open surgical operations, when keyhole surgery may be an option instead. - Aortic aneurysm screening Given the high risk of death following the rupture of an aortic aneurysm, most developed countries now offer a screening programme to detect these early for those at risk. These are male patients who are 65 years or older and those who are at least 50 years old with a first degree male relative (father or brother) who have had an aortic aneurysm in the past. Those with a long-standing history of smoking or difficult to control hypertension are also at risk of developing an aneurysm.
Screening is usually done by performing an ultrasound scan of the abdomen in those more likely to have one. Patients must starve for 6 hours before this scan, so a prior appointment is advisable. This allows detection of aneurysms in the aorta in the abdomen at a smaller size when the risk of rupture is much lower and for them to be followed up carefully and treated by keyhole surgery if necessary, before a rupture occurs.
An Ultrasound scan of the abdominal aorta is a non-invasive test that does not involve exposure to any radiation and can be performed in 20-30 minutes as a walk-in procedure at our vascular diagnostic laboratory at Gleneagles Hospital.
